5202 - Humerus, other impairment of
DBQ: Link to Index of DBQ/Exams by Disability for DC 5202
Definition
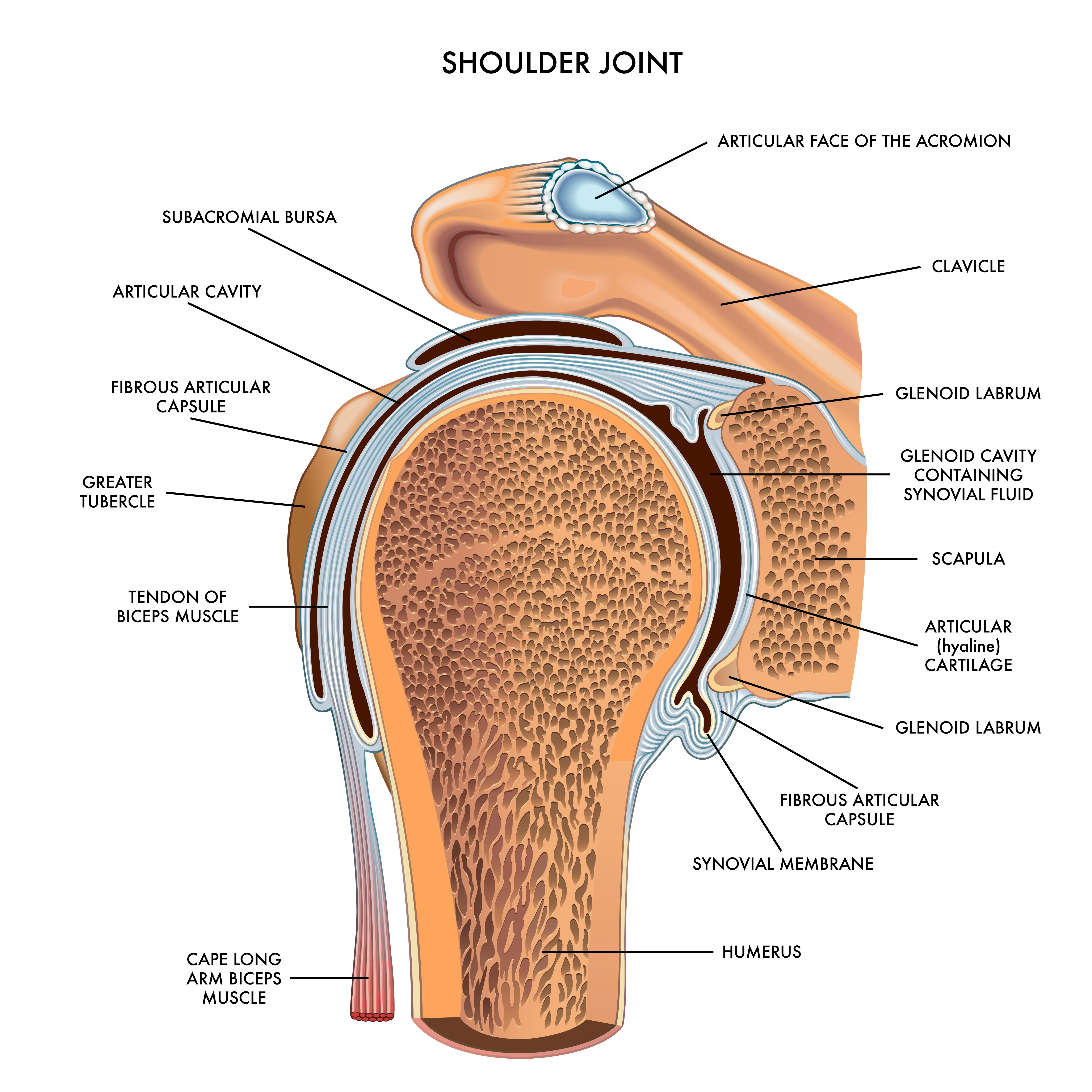
The humerus is the upper bone of the arm from the elbow to the shoulder joint. Impairment usually results in restrictive movement or range of motion (ROM) of a part, joint, or soft tissue, especially those imposed by disease or trauma.
{kind=link}
{kind=link}
Etiology
Restriction or excessive movement of the humerus may be caused by fracture, dislocation, torn muscle, arthritis, tumor, adhesive capsulitis (see Diagnostic Code: 5200 Scapulohumeral articulation, ankylosis of) or tendonitis.
Signs & Symptoms
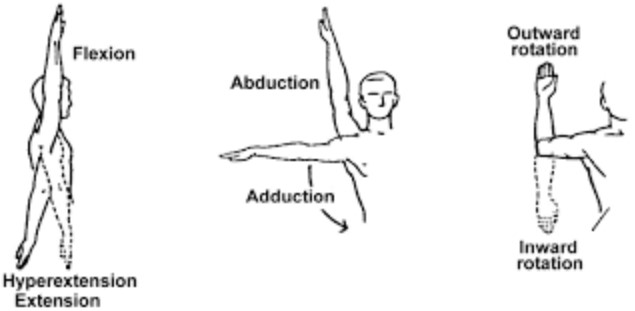
Manifestations of the impairment may include: limitation of motion; pain; a pop felt on external rotation of the shoulder; a flail joint which is excessively mobile due to paralysis of the muscles that control the joint; muscle weakness; or dislocation of the scapulohumeral joint.
Tests
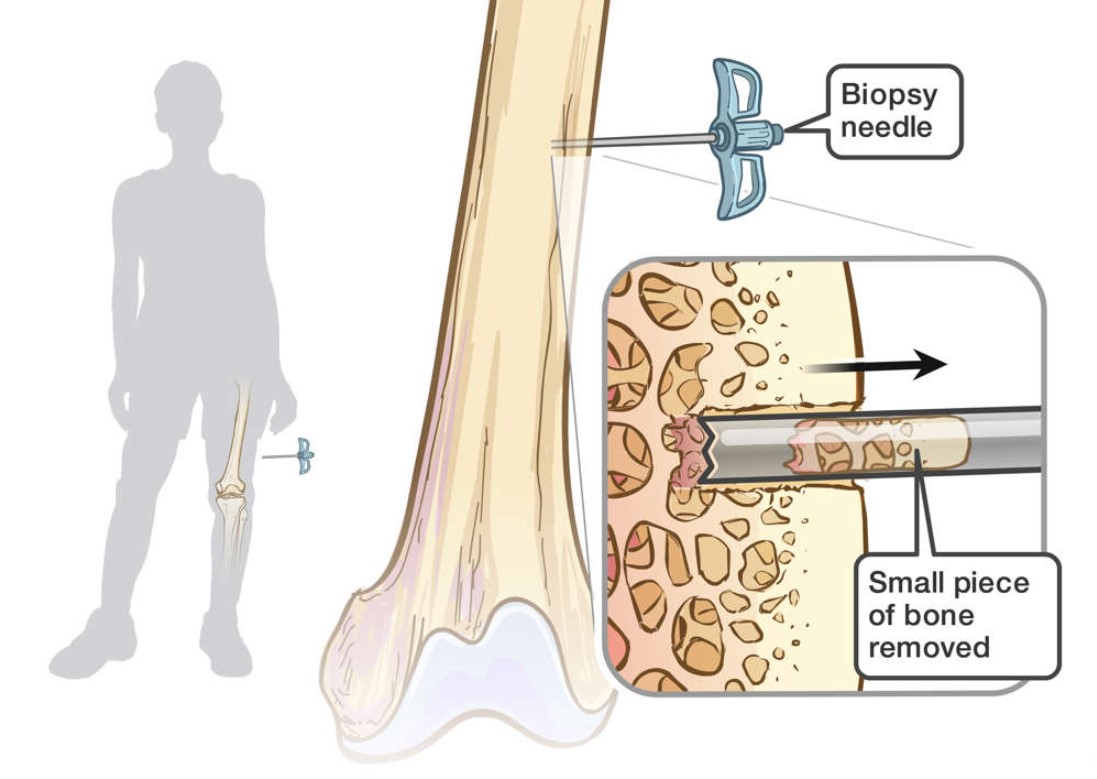
Tests that may be used to determine humerus impairment include: computed tomography (CT) scan, magnetic resonance imaging (MRI), bone biopsy, arthroscopy, x-rays, and arthrography.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment
Fracture treatment will depend on the type of fracture, and may range from immobilization with a splint or cast, to open reduction and internal fixation, to bone grafting. Dislocations are usually treated with immobilization and physical therapy. If conservative treatment fails for dislocations, then shoulder reconstruction may become necessary.
{kind=link}
{kind=link}
Residuals
-
Prolonged immobilization of joints may lead to stiffness and ankylosis. Wasting away of the bone may occur due to decreased usage and activity. The possibility of long-term rehabilitation exists.
-
When deciding expressly claimed issues, decision makers must consider entitlement to any complications that are within scope of the claim, including those identified by the rating criteria for that condition in 38 CFR Part 4. This could include but is not limited to, scars as the result of surgical intervention for an SC disability.
Special Considerations
-
The rating schedule for musculoskeletal was updated on February 7, 2021. Protection still does apply and should be considered with existing evaluations (38 CFR 3.951(a)).
-
Description of any instability and frequency of any dislocations is required.
-
Multiple precedential decisions have impacted the application of 38 CFR 4.59 for musculoskeletal disabilities. Refer to the table in the M21-1 for a listing of impactful precedential court holdings, a brief description of the impact, and the applicability date (date of decision) for each.
-
Separate evaluations may be given for disabilities of the shoulder and arm under 38 CFR 4.71a, diagnostic codes (DCs) 5201, 5202, or 5203 if the manifestations represent separate and distinct symptomatology that are neither duplicative nor overlapping. Refer to the M21-1 for examples of separate evaluations for disabilities of the shoulder and arm.
-
It is the responsibility of the rating specialist to interpret reports of examination in the light of the whole recorded history, reconciling the various reports into a consistent picture so that the current rating may accurately reflect the elements of disability present. See 38 CFR 4.2 – Interpretation of examination reports. If the report or examination is inadequate, the rating agency may return for a supplementary report. See 38 CFR 4.70 – Inadequate examinations. .
Notes
-
None.